

















































































Klevius lesson in genetics before you proceed to traumatics
Epigenetic changes consist of genes that are turned off and on as a result of experience and environment. It encompasses everything you or your parents have experienced.
Gene expression (the turned on gene due to environmental changes) changes in its daughter, granddaughter and even later. A classic example is how starving in one generation may result in obesity in the next so to build up body resources against starvation.
However, this is just trivial from a genetic perspective. Genes have to be both 1) long lasting, 2) varied and 3) adaptive . Therefore we have
1) a basic "backbone" of DNA that in
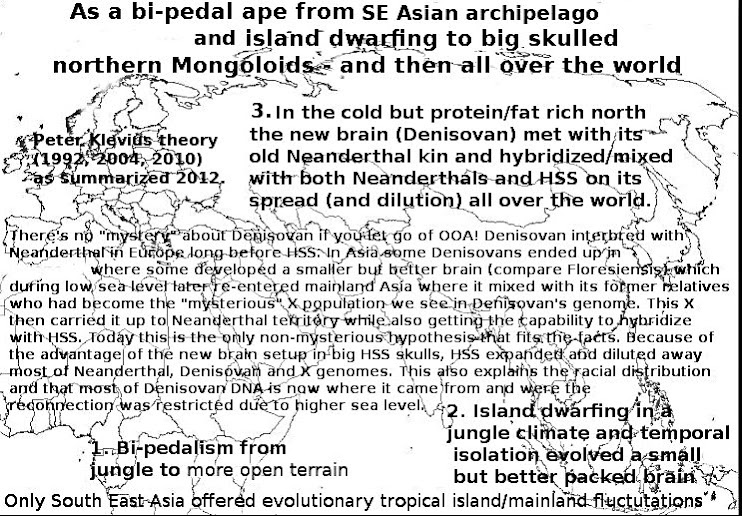
2) heterosexual reproduction is mixed to achieve diversity. No dude, difference in skin color etc single markers is no guarantee for more positive genetic diversity while too distant relationship bordering to hybridization may even cause more negative diversity - that's what happened after the Denisovan-X-Neanderthal-HSS swing party in Siberia at the birth of truly modern humans. Except for superior intelligence compared to other Homos, we also got an enhanced risk of genetic disorders. However, this tendency will probably level out at approximately the same pace as we all become more stupid over time compared to those guys who created the Denisova bracelet etc. due to the fact that we are so many now in a global society that peak intelligence will decrease due to lack of evolutionary niches. Moreover, due to religious reproduction steered by occultism and fanaticism, there is a filtering of intelligent people out from the "community" and their reproduction rate is usually much lower.
3) On top of this we have short term genetic "memories", also called epigenetics.
Together (+possibly more) these systems collaborate in all aspects of our lives.
Epigenetics affecting behavior means, for example, that certain methyl groups may repress the glucocorticoid receptor gene, making it unable to unwind from the histone in order to be transcribed, causing a decreased stress response. Stimulus then activate stress signaling pathways so to remove methyl groups from DNA. This in turn releases the actual gene and exposes it for transcription which results in lowered stress response.
Psycho-"scientists" claim: Holocaust survivors pass on trauma to their children’s genes.
For someone (like Klevius) acquainted with the history of psychology, psychiatry and psychoanalysis (rooted in exorcism) it's easy to trace the true motives/blind spots behind this kind of "research". Moreover, it's equally easy to see how this "research" interpretation clashes with huge studies of Holocaust survivors which showed no altering of personality despite horrifying experience.
Study finds that trauma suffered in lifetime can influence genetic make up of future generations
An N.Y. (the headquarter of stupid psychology/psychiatry incl. the powers behind the notorious DSM diagnostic bible) team carried out research on 32 Jewish men and women who had either survived a concentration camp, witnessed torture or had been forced to hide from the National-socialists (aka Nazis).
The "researchers" also examined the genes of the group’s children and compared the results with Jewish families who were living outside Europe during the Holocaust.
They found that there was a distinct difference between the two groups. “The gene changes in the children could only be attributed to Holocaust exposure in the parents,” according to a professor named Yehuda, director of the Traumatic Stress Studies Institute (the name of the institue already dismisses any seriousness in this "research").
Yehuda’s team was looking at a region of a gene which is both known to be affected by trauma and has a role in regulating stress hormones. This genetic “tag” was found in both the holocaust generation and their children. However how these tags are passed between the generations remains unclear.
Klevius comment: So! First of all, trauma is stress and therefore connected to stress hormones - compare Klevius discussion about cortisol and foster kids in Angels of Antichrist - social state vs kinship (1996):
In a recent and quite remarkable study, Flinn and England have shown how reduced kinship ties in the rearing environment increase children’s stress measured as cortisol levels. The results are impressive and support in every aspect closer and more extensive kinship ties, while at the same time they warn against leaving the child without such ties (Flinn & England 1995). With all due respect for the study, I am sure an Aborigine or a Bushman had known this thousands of years ago.
Secondly, these tags are jumping around all the time just like our immune system. Picking one out and declaring it a "traumatic" tag is sheer nonsense. But nonsense that sells!
Epigenetics affecting behavior
The first documented example of epigenetics affecting behavior was provided by Michael Meaney and Moshe Szyf. While working at McGill University in Montréal in 2004, they discovered that the type and amount of nurturing a mother rat provides in the early weeks of the rat's infancy determines how that rat responds to stress later in life. Immediately after birth, they found that methyl groups repress the glucocorticoid receptor gene in all rat pups, making the gene unable to unwind from the histone in order to be transcribed, causing a decreased stress response. Nurturing behaviours from the mother rat were found to stimulate activation of stress signalling pathways that remove methyl groups from DNA. This releases the tightly wound gene, exposing it for transcription. The glutocorticoid gene is activated, resulting in lowered stress response. Rat pups that receive a less nurturing upbringing are more sensitive to stress throughout their life-span. This stress sensitivity is linked to a down-regulation in the expression of the glucocorticoid receptor in the brain. In turn, this down-regulation was found to be a consequence of the extent of methylation in the promoter region of the glucocorticoid receptor gene.
This pioneering work in rodents has been difficult to replicate in humans because of a general lack of availability human brain tissue for measurement of epigenetic changes
Sir Michael Rutter*, the first professor of child psychiatry in UK
*) Rutter was the man behind a Holocaust survivor study that run straight in the face of psycho-dynamics.An early breakthrough was his discovery that autism, or infantile psychosis as it was then known, had a genetic basis, something barely suspected at a time when Freudianism and psycho-dynamics ruled.
The Isle of Wight Studies (1964-74) surveyed the mental health of children living on the island and for the first time in such research, children themselves were directly interviewed and questioned. Before this the assumption had been that what children thought and said didn't really matter.
In the 1970s, the Fifteen Thousand Hours study, delivered evidence about the combination of factors that affected the performance and behavior of children in inner city secondary schools. Findings from the study were included by both the Labour and Conservative parties in their 1979 election manifestos - albeit interpreted in opposite ways.
"Maternal Deprivation Reassessed" was Mike Rutter's challenge to John Bowlby's populist "theory" of maternal attachment.
Mike Rutter's fascination with the underlying reasons why and how children vary in their ability to weather and cope with adversity, led to the growth of resilience science.
Resilience is a term used to describe relative resistance to psychosocial risk
experiences. There is considerable variation in children’s responses to such experiences but research to determine the processes underlying the variations needs to take account of several crucial methodological issues. The findings emphasize that multiple risk and protective factors are involved and that children vary hugely in their vulnerability to psychosocial stress and adversity as a result of both genetic and environmental influences.
The overwhelming conclusion is that there has been a positive outcome for most children despite what is described as deeply traumatic experience.
For those interested, here's Michael Rutter interviewed by Normand Carrey in 2010 (Klevius will comment on this later):
Q. Tell me a bit about your family
A. I came from a very medical family. My father was a family doctor who at the end of his career became interested in public health and my grandfather was a doctor as well who was interested from the start of his career in public health. In addition, there was an uncle who was an eye surgeon. As a child, I became very aware that my father was regarded by both fellow GPs and consultants as outstandingly able. It was also obvious how much he enjoyed his work and it seemed natural for me to consider also becoming a medic.
I went into med school fully intending to be a GP and then join my father in his practice.
Towards the end of my medical training, I became interested in the relationship between brain and mind and in the clinical disciplines of neurology and neurosurgery. Accordingly, I settled on wanting to be a psychiatrist after training in the two neuro specialties. My father was initially disappointed I did not join him in general practice, but at no stage was he critical and he was always supportive of whatever decisions I made.
Q. You mentioned you were interested in psychology, prior to psychiatry?
A. At school I had read a lot of Freud and I was intrigued by that and I trained myself to wake up and write down my dreams. The person who taught me about Freud was a physics teacher, someone who actually was imprisoned for being a conscientious objector in the first world war. However later on, my views on Freud changed, radically.
Q. Tell me about internship, residency?
A. I did some psychiatry as an intern in conjunction with neurology and neurosurgery. As a medical student I had a period working with Professor Mayer-Gross, one of the major figures of German Psychiatry, who fled Nazi Germany because of his Jewish heritage. He was a wonderful teacher. I had vivid memories of my first case presentation to him.
He had me interview one of the psychiatry patients from the back wards but I could not make heads or tails out of this patient. In my presentation to him I said, “I’m sorry but I’ve completely failed you”. I was really convinced that I had entirely botched up the interview. He said let’s go through it. I described the hour and he showed me that I had made all the necessary observations for the diagnosis of hebephrenic schizophrenia. He transformed what I had perceived as a humiliating failure into a positive experience. Of course, it was a pseudo-success because I had not understood the significance of what I had observed. Nevertheless, it was spectacularly good teaching. He asked searching questions but designed in a way to focus on my successes. Later, he advised me that I should go into psychiatry but to do some general medicine and neurology before hand. That would be impossible to do now because you are supposed to settle on your specialty the day you graduate, a totally silly idea.
So I did that before going on to do psychiatry at the Maudsley. However I hesitated about the Maudsley because the expectation was to do a research project and I was worried because I thought I would be useless at research and I would end up hating it. Of course I was wrong on both counts. I was reasonably good at research and I enjoyed it tremendously.
The point is that Dr. Mayer-Gross knew more than I did about what I could and should be doing, more so than I.
This was mirrored by my next mentor, Aubrey Lewis at the Maudsley who decided I should become an academic child psychiatrist, something that scarcely existed up till then. My job, according to him, was to put child psychiatry on a solid research basis, even though he was an adult psychiatrist himself. I was not keen on the idea, but because of his encouragement, I said that I would give it a go. It was not obvious to me, at least at that point how child psychiatry could be made better. Aubrey, unlike other contemporary academic adult psychiatrists, had a vision of the importance of developmental approaches and the need to understand the continuities and discontinuities with mental disorders in adult life. I shared that vision but was reluctant at first because of the general muddledom that pervaded the clinical discipline of child psychiatry at that time.
Aubrey Lewis was a terrific teacher. People were afraid of him because he was a polymath who seemed to know everything. For example, if you had a patient with a certain rare religion he knew about that, or if the patient was a poet he knew about that as well, and he was able to discuss these various topics at a very high level. He came across as intellectually intimidating but he was very good to me, he gave me compliments about my abilities that I had not received before and he provided me with career opportunities. He was right that child psychiatry would suit me; its just that I had not realized it up to that point. He fostered research and most professors of psychiatry in the UK at that time trained under him.
One of the things I learned through this is that the modern idea that everyone should choose what they want to do is not always right. There are times when you should have an experience that you would not necessarily have chosen but which is relevant, which in my case it was.
Q. Tell me a bit about your childhood, you were around 6 years old when the war started?
A. I was born in the hills of Brummana, in the hills above Beirut. I came to England when 3 years old, as fluent in English as in Arabic, which I’ve completely lost. In 1940, my younger sister and I were evacuated to live in two separate families in the same town in the US because my parents feared, like everyone else, that England would be invaded imminently by Hitler. I was sent to a very nice American family, friends of friends of my parents and they did a wonderful job in keeping my English family alive in my thinking. My parents wrote letters once a week but the mail came in dribs and drabs according to when it got through. Although it sounds a bit odd I never felt separated from my original parents. People think I should feel a loss but all I can say is that I didn’t. My new foster parents were punctilious in not taking over from my parents. I called them aunt Mary and uncle Dick but they were actually my parents for that four year period in America and I’m still in touch. My American father has passed away but my American mother whom I saw 2 weeks ago is close to 100. I also see my “foster sibs” from time to time; the next occasion will be in August.
That was an important period, which so far as I am aware had no negatives, I was happy there. I think my parents were more upset than me because given that Hitler did not invade they felt guilty about their decision. I left as a responsible 7 year old thinking of myself in charge of looking after my younger sister. It is interesting how one’s self-image is affected by social context. Four years later I returned as an ebullient American teenager. I remember my grandmother saying to my mother, “Winnifred, do you think we’ve got the right ones back”. The re-entry for me was a very easy one. Four years is a long time, the person that came back was not the same person who had left. By contrast, although much had happened during the 4 years that I was away, my parents were just as I remembered them.
Q. Tell me a little about your sister who went with you?
A. My sister also came but she was in a different family in the same small town. Initially I saw a lot of her but then her foster mother became pregnant and decided she could not keep my sister. I think that was cruel and insensitive and not necessary, because they were reasonably well to do, and only had one other child. The family I was with requested permission from the authorities to have my sister and they were told they could not do that (that would have been 4 children but there was ample space). The social workers who made these decisions had no understanding of the needs and feelings of young children, that was a ridiculous decision. She was sent to another family and was not very happy there. Eventually, near the end of the four years, social workers decided, before we were to return to England that she could live with me for a few months because we did have to get to know each other again.
Q. Any link between these childhood experiences and your choice of child psychiatry and the issues/themes you have been attracted to (ie Bowlby’s emphasis on separation, Romanian orphans, resilience)?
A. No I don’t think so. I’m not aware that any of that played any role in what I decided to do subsequently. You may well find that surprising, because looking at it from the outside it seems fairly obvious that it might have provided a research interest in attachment and separation. Perhaps it may have had an impact at the unconscious level, but I’m not aware of it.
What I did learn was that I could be happy in other places. The concept of my country right or wrong has always alienated me. England has always suited me, but if it ceased to do so, I would have no difficulty moving to the US.
Q. Tell me about your relationship with John Bowlby.
A. At the time I wrote “Maternal Deprivation Reassessed”, I had heard him talk but did not know him personally. His supporters were critical of me with respect to what they perceived as my attack on Bowlby. However, I was simply raising important issues and I think he saw it that way too. Later on I got to know him better and of course his own research into children admitted to TB sanatoria showed that they did not suffer in the way he postulated, so he recognized that separation was not as damaging as he had initially thought. He was an honest man, so he took those findings on board and changed his thinking accordingly. He was a pioneer in bringing together a diverse group of people including animal researchers like Harry Harlow, Robert Hinde as well as psychologists and psychoanalysts, although he was not enamored with epidemiology. He started with the view that in understanding behavior you had to look at a wide range of evidence; in those days for a psychoanalyst to take such a broad perspective was unique. His first volume of his trilogy on attachment was vitriolically attacked by psychoanalysts. Later on analysts realized he was a good thing for them and wanted to adopt him as one of their own. Interestingly Bowlby himself in his first volume was very firm in terms of the importance of psychoanalysis in what he wrote but in 1988 he said that psychoanalysis was never more wrong than in its theory of child development, so he became more distant from psychoanalysis, in some ways and not others. He, like me, remained positive about mental mechanisms but he regarded the theory of psychosexual stages as “total bunk” and it was. “Total bunk”; those are my words, not his but that is more or less what he thought.
Attachment theory was a major contribution to child psychiatry, and there is no doubt he put it on the map in a thoughtful way. Firstly he saw the need to understand social relationships. He postulated that the selective attachment between baby and mother was special in a sense in that it later became the base for love relationship, close friendships and parenting but different from other types of interactions such as play behavior, important for learning in children. This was a very important distinction he made. He also emphasized that selective attachment had a functional role of providing a source of security, and secure base, and both human and animal evidence have amply confirmed that view.
The films of children admitted to hospital made by James and Joyce Robertson made a huge impact and although it took time, they forever changed people’s ideas about what was important when admitting children to hospital. In fairness the films, because they were so vivid, were as important as Bowlby’s theorizing; the two of them together were a powerful combination. Where Bowlby was misleading in his initial writings was seeing this all in terms of the exclusive mother-child relationship, saying it was different from all other relationships; evidence shows that this is not always the case; children are capable of more than one selective attachment and it is advantageous for children to have more than one so that if something happens eg there is a death in one of the main attachment figures, then they have other relationships to turn to.
Q. What is your view about theorizing?
A. My research is and should be hypothesis driven. Peter Medawar, the Nobel prize winning scientist talked about science telling a story. There are the empirical phenomena that have to be explained. The scientist puts forth a hypothesis, a mini-theory, of the mediating variables that he/she is studying, postulating initially the variables having a causal effect but then proceeding to the empirical research to test the hypotheses. The result may show that the hypotheses were partially right, sometimes partially wrong, or occasionally totally wrong or totally right. The need then is to revise the story and then go back to empirical testing. If that is what is meant by theory then its central.
What theory in psychology has tended to mean however is something that explains the whole of life; psychoanalysis did that, then behaviorism and in modern times genetic determinism. There should be a plague on all of those because they have held back understanding as a result of taking the role of religion. In a paper that is coming out soon I equate the role of psychoanalysis in relation to psychiatry as equivalent to creationism in relation to evolutionary theory. The trouble is not deciding if claims are right or wrong; it is more that there has to be an appeal to some authority, rather than turning to facts or logic. I think that has held psychiatry back for a long time.
Q. Tell me about the impact of your semimal papers; the Isle of Wight studies, the maternal deprivation monograph, the 1987 paper on Psychosocial risks. They seem to have an appeal that goes beyond the good solid science they were based on.
A. I’ve done different sorts of research at different times but the things in common across the papers you mentioned is that in many I had been interested in policy implications and many have involved collaborations in the field. The school studies had a lot of input from teachers. That was extremely valuable and not just a courtesy; teachers could point out where we were drawing wrong conclusions about our inferences and we took this feedback into account in writing our papers.
Also we attempted to make the research reasonably accessible and policy relevant, not just in sense of usual government policy but more in the sense that these are the issues and concepts that you have to think about in terms of what you are going to do with the findings. It has been important to me to help researchers understand what policy makers have to do and conversely how policy makers have to understand how research works.
One of the things we found was that the average class size does not matter at a time when teachers were opposed to increasing class size. One of my more frightening experiences was when I had to give a talk to the Federation of Teachers; I thought they were going to seize on my findings and tear me apart limb by limb. After my presentation the first teacher who spoke said that my message was in fact liberating; she said what you are saying, Dr Rutter, is that we should forget about the average class size and concentrate on areas where class size makes a difference-ie for young children learning to read and for children with handicaps. Teachers rightly saw this as giving them a license to decide about class size according to the needs of the children rather than just following some arbitrary dictate from above.
Q. What attracted you to the Romanian orphan issue?
A. The British department of Health had become aware of a substantial number of orphans coming into the country and the government had nothing to go on to base treatment. We did an initial 6 month pilot and there was enough there to justify going on to a bigger study, a study that combined the scientific questions that could be answered from such a natural experiment and the information we needed to inform treatment. It is one of the more interesting bits of work I’ve done since it was so full of surprises. And it is the surprises that make research so addictive.
Recently we have had two publications linked to this work, an SRCD monograph which is an academic publication, written for researchers, and another one published last September by BAAF (British Association for Adoption and Fostering) on the 45 questions most often asked about the findings, deliberately written more from policy and practice point of view. The style in these publications is different but written from the same data.
The Romanian orphan issue became politicized when some newspapers were suggesting that some orphans were being sent back. We knew that some families were having difficulties but not a single orphan in our study had been sent back. We decided to go public with this. The newspaper that published the initial story, in my opinion, was being dishonest in suggesting that multiple children had been put back in Romanian institutions.
Q. Is there one patient that stands out for you, that had more of an impact on you?
A. One is an adult patient whom I saw following a suicide attempt in prison. He had a terrible upbringing and first came before the courts as an out of control five year old. He went through various institutions and landed up with a quite severe charge as a youth. On release he met up with a young woman from a very different background. This was followed by him totally giving up crime and leading a productive life, getting a job, and getting married. The suicidal attempt came when his wife died in child birth and he went to pieces, engaging in a spell of setting fires to buildings in a state of anger.
It raised the question for me-had he recovered or had he not? The answer I came up with was yes he had recovered (before his wife’s death); had it totally changed him-no.
Thinking about resilience this case certainly made an impact on me, it made me think, we must get away from thinking about resilience in absolute terms, in terms of a total turn-around; that can occur but it is relatively uncommon.
Q. Were you in the middle of your resiliency work then?
A. No this happened to me before that, quite a long time before that; my writings put resilience on the map but I was not the first one to use the term, I don’t think so.
Q. You still see patients? Why? You don’t really need to,…
A. My clinical work since I retired 12 years ago is entirely derived from my research patients; I see Romanian adoptees and individuals with autism whom I first saw as children, themselves close to retirement, or new cases of autism which are puzzling.
I enjoy clinical work, and I enjoy the challenge; these are difficult cases, I have to make sense out of them.
In order to continue working I have to show to the College that every year I have 50 hours of CPD (continuous professional development), a legal requirement to maintain my license in order to see clinical patients. Given the high co-occurrence of autism with other conditions, I have to keep up to date with other associated conditions such as ADHD, and up to date with treatments such as psychopharmacology and psychological therapies.
Also I have this firm view that if people are helping you with your research then you have a duty to help them in return when they run into difficulties.
Q. So there a lesson in humility in there for the rest of us?
A. Yes, I suppose so.
Q. Was the knighthood a surprise? That they would recognize a child psychiatrist?
A. You never know precisely why you get it. The minister who played an important role was the minister of education (Keith Joseph) because he was impressed with how I was trying to make education research relevant.
It’s pleasant to get it but the title is not anything I use, everyone knows me as “Mike” whether fellow professionals or the cleaning staff.
What meant much more to me was the election to the Royal Society (in England), the top scientific accolade-at that time I was the only psychiatrist in the Society, in recognition of my science and clinical work.
My nomination to the Institute of Medicine in the United States National Academy of Sciences, an institute concerned with policy and practice was similarly very satisfying for me.
Q. You set up the MRC Child Psychiatry Research Unit, and the Social, Genetic and Developmental Research Centre?
A. It’s too much of a mouthful, I’ve tried to shorten the title but I do see that as one of the most important things I’ve done because it brings together genetics, psychosocial research and developmental research, I had seen this as a need since the 1970’s.
Q. Any comments on the two classification systems, ICD vs DSM?
A. What I say now is as an individual rather than a representative of WHO or APA, because I chair the working party on ICD dealing with child psychiatric disorders.
My view is that they both have similar sets of strengths and weaknesses. Both organizations are very bureaucratic and although both talk about the decisions being driven by science, I would simply say that I remain to be convinced that that actually happens.
We have a system, in both cases where there are far too many diagnoses; there is no way any psychiatrist can remember the algorithms for hundreds of diagnoses, so what do psychiatrists do? They opt out by diagnosing NOS, which means that the individual psychiatrist is thinking “I don’t believe in the differentiation” or “I couldn’t be bothered with it”. Either way, as a piece of scientific information, it is useless.
So I’m hoping that the new classifications will have a radically smaller number of diagnoses. I would also like to see the abolishment of all the separate categories for childhood onset disorder and replace that with having within the criteria for all psychiatric disorders explicit criteria dealing with varying manifestations within the disorder ie making the developmental features more apparent.
Q. Was the child classification in the DSM or the ICD a “hand-me-down” from the adult classification?
A. The two things are somewhat different-DSM tries to combine a research and clinical classification, whereas ICD has them separate. In my view there is no question ICD is right, the needs are different.
The other issue is that ICD is starting, for the first time, to plan for a classification for use in primary care. In the old days they developed a complicated classification for the specialists and then you boiled it down for the non-specialists. Now they are attempting the opposite saying the basis should be what is needed for primary care or in the case for child psychiatry, non-medical primary care ie school counsellors, social workers, pediatricians, the object being some 20 diagnoses not umpteen hundred. Will that be successful, I don’t know but it’s a good idea.
Q. Any comments about your colleagues- we know the impact you have had as a mentor, what about the opposite, the impact of colleagues, mentors on you?
A. I place a very high premium on mentors. I have been exceptionally fortunate in having excellent mentors throughout my career. Interestingly, with one exception, they were not child psychiatrists. Aubrey Lewis of course, then Jack Tizard, the social psychologist, Birch the American comparative psychologist, Robert Hinde the animal researcher and ethologist and Lee Robins the sociologist. The one exception was Leon Eisenberg, a child psychiatrist who was a good friend and important mentor. Norm Garmezy at a later stage was an important mentor in relation to resilience and development psychopathology. What you may have noticed is that none of these people have worked directly with me so that is saying you need to choose your mentors regardless of whether or not they are in same institution. You need to have a mentor who is tough minded, critical, but equally who respects your views and gives you the scope to make your own mistakes. A mentor will protect you from making disastrous mistakes but recognizing that you learn by doing and all the people I’ve mentioned and in recent times, Terry Moffitt and Avshalom Caspi, all have that quality, enormously supportive of their younger people. I add two things- do not go to a control freak because you won’t get the freedom to do things and don’t go to someone who insists on having their first name on the paper because a paper with an international star on it whether the international star is first or fourth or last, you remember that whereas the more junior researcher who has done all the work, won’t have his or her name remembered unless they are first author. That is a key issue. Yes I’ve learnt a lot from other people and my success owes a lot to their input.
Q. Is child psychiatry a true field like we would define physics or chemistry or a clinical field like cardiology, or is it a series of practices since it needs to borrow from other fields ie social sciences on one side and then basic sciences, ie genetics, neurosciences on the other side?
A. Let me answer that indirectly. One of the things that have changed beyond recognition are the divisions among the different branches of sciences. Biochemistry and genetics had nothing to do with one another a generation ago whereas now they are more or less the same field. The same would apply to many other fields. What about physics? Many of the leaders of molecular biology were physicists, and they came into the field because they recognized the real challenges were in biology and they were responsible for some of the major advances. The divisions are going if not gone, I don’t mean entirely gone but you have to understand enough of the others to make sense of things.
What about child and adult psychiatry-should those be separate? The research tools are the same so I see the desirability of close links in training and practice but one thing that is different is the developmental emphasis. Now that is less different than it used to be. I remember one of the leaders in the field saying why on earth are you talking about development in relation to psychiatry, schizophrenia is an adult disorder. However, researchers like Robin Murray and Danny Weinberg have shown and persuaded people that the developmental origins of these disorders are absolutely crucial. It would still be true that the developmental approach should be crucial in child psychiatry. Why do I say should be rather than is, because I am appalled that so few child psychiatrists are active in the Society for Research in Child Development. The issue of development has changed in two respects, one is the life span perspective and now when you talk about development you mean biology as well as psychosocial experiences as well as public percepts. So one might say that this is the reason for child psychiatry to have relative independence and the training should reflect that.
What about pediatrics? Winnicott infamously said you did not need any training in child psychiatry, all that was needed was to be trained in pediatrics and have a training analysis. Pediatricians I see as closely related in clinical work, less so in research but what they don’t know about is families; it’s not part of their training.
Do any one of those things I mentioned, individually, provide sufficient justification for separateness? No but I think in total they do. But I am not in favour of a competitive separateness. I have always had close links with adult psychiatry and pediatrics.
Q. You had two periods abroad, one year in New York, one year in California. Were they sabbaticals? Were they helpful?
A. They were not funded sabbaticals because British med schools don’t fund sabbaticals, so I had to fund my time abroad and find a replacement but yes they were sabbaticals in the sense I didn’t have ongoing clinical responsabilities.
Both were tremendous formative experiences. In New York I worked with people like Stella Chess, Alex Thomas and Herb Birch. They seemed to know everyone who mattered in the field and brought me in touch with Jerome Kagan, Lee Robins, and Ed Zigler among others; so I came away having made working relationships and friendships with the leaders in the field and they were enormously kind to me.
In Stanford I was in touch with Herb Lieberman, Judy Wallerstein, Jerry Patterson, Lew Lipsett, and we got to know each other well and our spouses also got along well, a good bonding experience.
Q. You have never followed the herd, now everyone is coming around to your point of view, what have you done, what accounts for this,?
A. I’ve always been an iconoclast- I’m a non-joiner, I didn’t join psychoanalysis or behaviorism and I see that as an essential quality to become either a good scientist or a good clinician.
Why have many of my ideas been taken up? One is my ability to be a synthesizer across disciplines but at the end of the day, data win through. Of course there are rivalries that impinge on everybody, but people do get persuaded when the evidence requires it and so it should be.
Q. Any predictions for the future?
A. I’m optimistic but with guarded optimism. There are too many claims made about major breakthroughs if not this year then next year and I think that is not realistic.
I worry about how economic motives come in, I worry about the narrowness of some of the research, but on the other hand we have concepts and technology available that were inconceivable when I entered the field so the possibility of doing really important things have gone up.
In the UK and the US, I don’t know about Canada, what has gone up is the bureaucratic demands on time so that you have to take on much more in the way of onerous administrative responsabilities.
Q. Ending comments?
A. I don’t have any regrets, some things have worked out better than others yet some of the rebuffs have been helpful. At an early point in my career I was in line for a job in general medicine but did not get it due to political considerations but instead I got a better job in pediatrics. I did pediatrics at a time when I had no idea I was going to do child psychiatry. I learned a lot about children from that. Not getting the first job was a blow to me at the time, but in retrospect, I’m glad I did not get it.
It’s been an exciting career, I could not have chosen one that suited me better, it’s the particular mix of things I’ve been able to do, both interdisciplinary, combining clinical and research work and the many international collaborations and contacts.
Thank You Dr Rutter.